

The phrase technical debt is used broadly in NHS digital strategy conversations, but what it actually means in practice for a large acute Trust is often poorly understood. It means SQL Server instances running versions released before the iPhone existed. It means databases that nobody has documentation for but that clinical and operational processes depend on every day. It means infrastructure that cannot support the analytics, AI, or FDP integrations that are central to every NHS digital business case written in the last five years.
Managing legacy technical debt in NHS data environments is not glamorous work. It does not have a procurement framework named after it. It does not generate the same executive attention as EPR go-lives or AI pilots. But it is the foundational prerequisite for almost everything else NHS digital programmes are trying to achieve. And in 2026, the SQL Server end-of-support timeline has made it urgent in a way that is now measurable and enforceable.
The Scale of the Problem
NHS Trusts are not unique in carrying SQL Server legacy debt. But the combination of factors that shapes the NHS context makes the problem particularly acute. Decades of system procurement conducted at departmental and Trust level, without consistent architectural standards, has produced data environments with SQL Server instances spanning multiple versions, many running applications that have no migration path defined, some running applications whose original developers are long gone.
Discovery exercises conducted in large NHS Trusts consistently find SQL Server estates that are larger and older than IT teams believed. Instances are found on servers that are not in the formal asset register. Databases are found that are connected to clinical systems and processed daily by operational teams but known to nobody in the IT function. The estate that can be managed is the estate that is known. The estate that cannot be accounted for presents an unmanaged risk.
The healthcare sector globally reflects the same pattern. Research from HIMSS Analytics found that over 60 percent of hospitals still operate at least one critical application on legacy software that lacks cloud-readiness or modern API interoperability. NHS Trusts running hundreds of distinct clinical and operational systems face this challenge at scale.
Legacy technical debt in NHS data environments is not primarily a technology problem. It is a visibility problem. You cannot manage, migrate, or decommission what you do not know exists.
The SQL Server End-of-Support Timeline: What Is at Stake in 2026
The SQL Server end-of-support timeline provides the clearest, most immediate forcing function for legacy debt remediation in NHS data environments. The table below sets out the current position for each version.
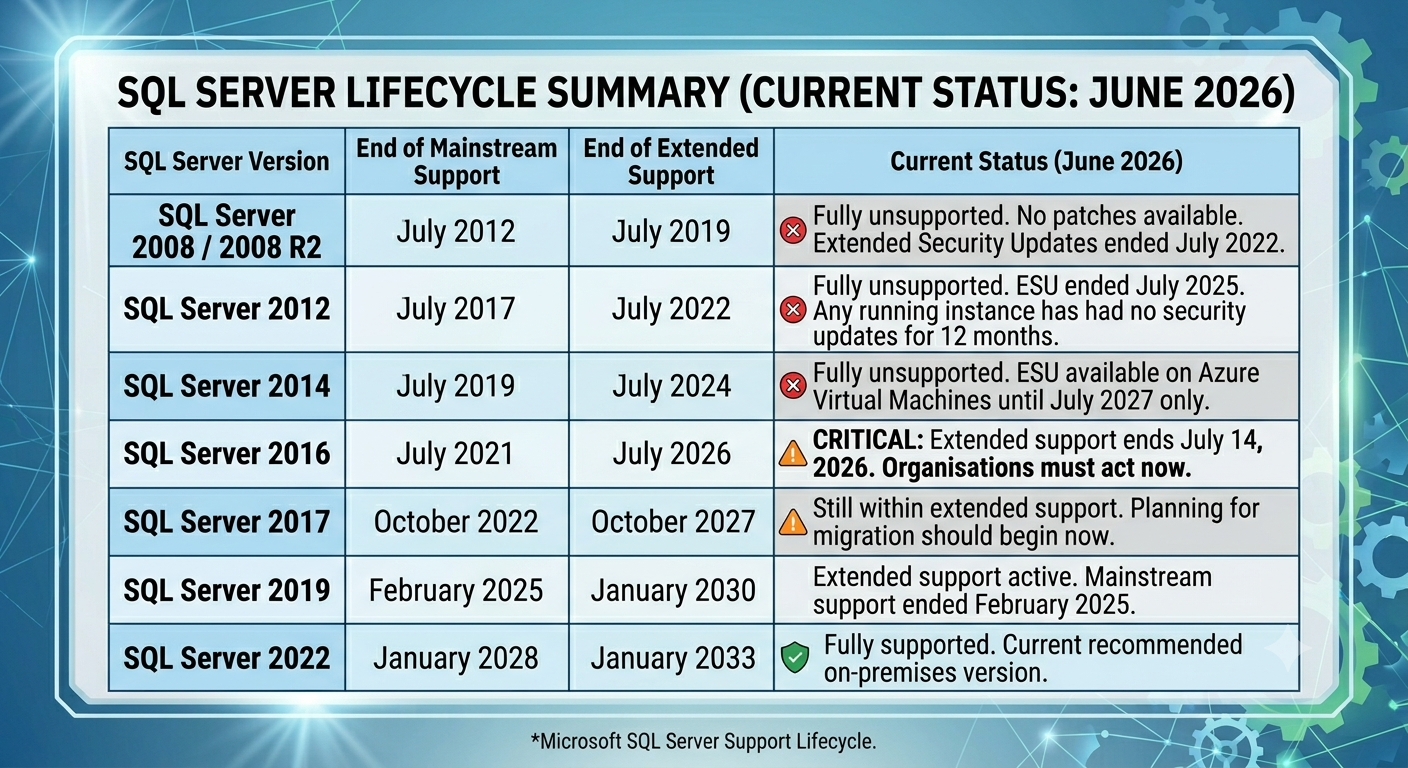
The most pressing deadline is SQL Server 2016, which reaches end of extended support on 14 July 2026. For any NHS Trust still running SQL Server 2016 instances that have not been migrated or covered by a formal Extended Security Update arrangement, that date represents an active compliance and security exposure.
SQL Server 2012 is the more alarming situation for Trusts that have not yet audited their estate. Extended Security Updates for SQL Server 2012 ended in July 2025. Any instance running SQL Server 2012 today has had no security patches available for twelve months. It is, in practical terms, a permanently unpatched database server running in a clinical environment that handles patient data under UK GDPR and DSPT obligations.
SQL Server 2008 and 2008 R2 are even older. Extended Security Updates ended in July 2022. Instances of these versions found during discovery exercises in NHS Trusts are not theoretical occurrences. They exist. They are running. And they represent the accumulated consequence of years of deferred migration decisions.
Why This Is a Compliance and Governance Issue, Not Just a Technical One
DSPT Alignment with the Cyber Assessment Framework
The 2025/26 DSPT cycle introduced full alignment with the NCSC Cyber Assessment Framework, representing the most significant change to NHS data security compliance since the toolkit launched in 2018. The shift moves NHS organisations away from checklist-style self-assessment towards outcome-based, evidence-driven assurance. Mandatory independent audits are now required for Category 1 and Category 2 organisations.
Under the CAF-aligned DSPT, vulnerability management is a core assessed area. Running unsupported SQL Server versions on which no security patches are available is a vulnerability management failure that cannot be papered over with a policy document. Evidence must be demonstrable, not declarative. A Trust that cannot show it has a documented programme for addressing unsupported database software is exposed in its DSPT submission in a way that was not previously visible.
NHS Data Security Standard 8 requires that the Senior Information Risk Owner is personally informed when systems cannot be upgraded, and personally signs off on the risk treatment or tolerance decision. A SIRO who has not been informed about SQL Server 2012 or 2016 instances in the Trust's estate cannot have applied that standard. Which means the standard has not been applied, and the DSPT evidence for it is incomplete.
UK GDPR Security Principle
Article 5(1)(f) of UK GDPR requires that personal data is processed in a manner that ensures appropriate security, including protection against unauthorised or unlawful processing and accidental loss. The ICO's guidance is explicit that this includes actively managing software vulnerabilities and using in-support software. Running patient data on unsupported database software is not a risk that can be indefinitely tolerated. It is an active compliance exposure that the ICO can and does take into account when investigating data security incidents.
The 2017 WannaCry ransomware attack, which cost the NHS an estimated £92 million, cancelled around 19,000 appointments, and disrupted clinical services for weeks, was made possible by unpatched vulnerabilities on systems running software for which updates were available but had not been applied. The attack exploited precisely the category of vulnerability that unsupported SQL Server instances present today: a known, unpatched weakness in an internet-connected clinical environment. The lesson from WannaCry was absorbed at the time. The conditions that made it possible are present again in NHS Trusts running end-of-life database software.
What the Technical Debt Actually Costs
The temptation to defer SQL Server migration is understandable. Migration consumes programme resource, involves application dependency analysis, risks disrupting systems that clinical operations depend on, and produces no visible new capability. The cost of not migrating is less visible, which is why it is consistently underweighted in NHS digital prioritisation decisions.
Direct Security Exposure
Once a SQL Server version loses support, vulnerabilities discovered after that date receive no patches. The attack surface is permanent and grows over time as new vulnerabilities are identified. The security difference between a supported and an unsupported SQL Server instance is not theoretical. It is the difference between a system that gets patched within 14 days of a vulnerability disclosure, as NHS Data Security Standard 8 requires for high-risk vulnerabilities, and a system that can never be patched regardless of the severity of what is discovered.
Increasing Migration Complexity
Every year that migration is deferred, the migration becomes more complex and more expensive. Application dependencies accumulate. The SQL Server version gap between the legacy instance and the target platform widens. Compatibility testing requirements grow. The people who understand the original configuration move on. As one industry analysis puts it bluntly: the version gap widens, the institutional knowledge fades, and the person who set it all up has long since left. The cost of migrating SQL Server 2016 to Azure SQL Managed Instance today is materially lower than the cost of migrating SQL Server 2008 will be in three years.
Blocked Transformation Programmes
Legacy SQL Server estates are consistently the constraint that slows NHS digital transformation programmes. EPR data migration exercises discover dependencies on old SQL Server instances that were not in scope. FDP integration work is blocked by databases that cannot expose data via FHIR or modern APIs. AI and analytics pilots cannot use data that is trapped in unsupported, undocumented, un-integrated legacy databases. The technical debt does not sit passively in the background. It actively prevents the programmes that NHS Trusts are investing in.
The Migration Options
For NHS Trusts addressing SQL Server legacy debt, the migration decision is not binary. The appropriate path for each database or instance depends on its workload type, its application dependencies, its clinical latency requirements, and its long-term role in the Trust's target data architecture. The table below summarises the main options.
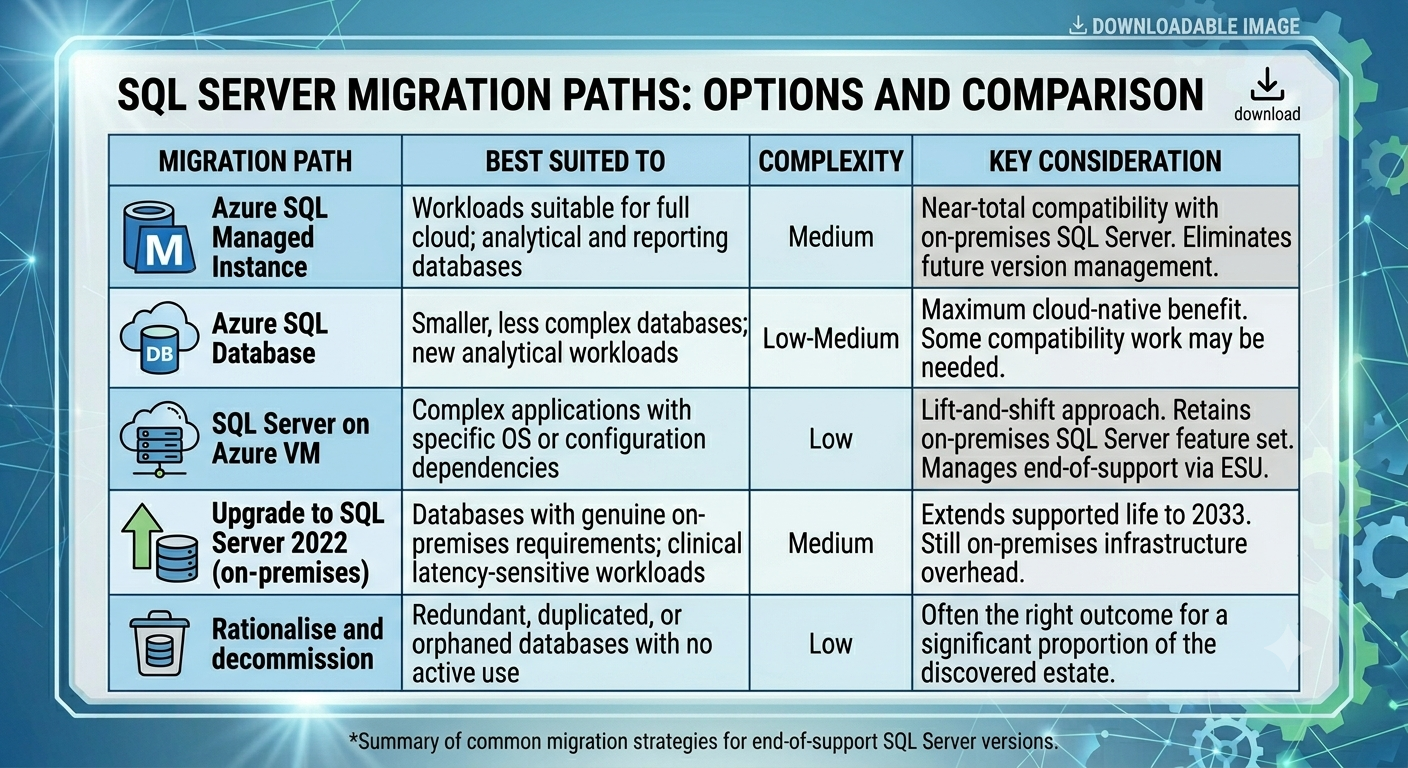
For most NHS Trusts, the outcome of a structured assessment will be a mixture of these paths. Some databases will migrate to Azure SQL Managed Instance as part of the cloud data platform build. Some will be hosted on Azure Virtual Machines as a stepping-stone to full migration. Some will be upgraded to SQL Server 2022 on-premises where genuine clinical latency or connectivity constraints make cloud inappropriate for now. And a meaningful proportion, often larger than expected, will be rationalised and decommissioned because discovery reveals they are orphaned, duplicated, or no longer required.
How to Approach the Programme
A structured programme for addressing SQL Server legacy debt in an NHS Trust follows a consistent sequence. The specific detail varies by Trust, but the logic is the same in every case.
Discovery First
Automated network scanning to identify all SQL Server instances across the estate is the essential starting point. Asset registers and IT team knowledge systematically under-count the true number of instances in large NHS Trusts. Automated discovery tools can identify instances by network signature, SQL Server version, database inventory, and connectivity patterns. The output is a complete, evidence-based inventory of what exists, what version it is running, what databases it hosts, and what systems or applications are connected to it.
Discovery is also the point at which orphaned databases are identified: instances that appear to be running actively but for which no application dependency or operational use can be confirmed. These are migration candidates that can be decommissioned without the application compatibility work that active databases require.
Risk-Based Prioritisation
Once the estate is documented, prioritisation is straightforward in principle. Instances running end-of-life versions that hold patient-identifiable data are the highest priority. Instances running end-of-life versions that are internet-facing or connected to clinical systems are the next priority. Instances running still-supported versions but approaching end of support in the next 18 to 24 months should be in active planning. Instances that are entirely internal and hold no patient data have lower but still real compliance exposure.
This prioritisation should be documented and presented to the SIRO as the formal risk treatment plan that NHS Data Security Standard 8 requires. The plan should include timelines, resource requirements, and interim security controls for instances that cannot be migrated immediately.
Migration Sequencing Aligned to Wider Architecture
SQL Server migration does not happen in isolation. The target destination for each database is shaped by the Trust's wider cloud data architecture design. Databases that will become part of the cloud analytical layer should migrate to Azure SQL Managed Instance or Azure SQL Database. Databases that support clinical systems with latency requirements may need to remain closer to on-premises infrastructure during the transition. Databases that support EPR-adjacent applications should be sequenced around the EPR programme to avoid competing demands on the same teams and systems.
This is why SQL Server rationalisation is best designed as a workstream within a broader enterprise data architecture programme rather than as a standalone IT project. The migration decisions are architectural decisions, and they need to be made in the context of the full target architecture rather than optimised for each individual database in isolation.
Decommissioning as Outcome, Not Failure
The most underutilised outcome in NHS SQL Server legacy programmes is decommissioning. Discovery consistently reveals databases that were created for specific purposes years ago, whose original purpose has been superseded, and that continue to run on infrastructure simply because nobody has confirmed they can be turned off. Rationalising these databases reduces the estate, reduces the attack surface, and reduces the ongoing cost of maintaining infrastructure.
Treating decommissioning as a legitimate and positive outcome, rather than as a failure to find a migration path, is a cultural shift that NHS digital leaders need to actively encourage within their teams.
The July 2026 Deadline Is Not the End of the Story
SQL Server 2016 end of support in July 2026 is the most immediate deadline. But the principle it represents applies to the full legacy estate, not just to a single version. SQL Server 2017 reaches end of extended support in October 2027. SQL Server 2019 mainstream support ended in February 2025. The pattern of accumulating legacy debt, deferred migration, and compounding risk does not end with a single programme. It requires a sustained architectural discipline that treats database versions as assets with lifecycles, and plans migration as a continuous process rather than a crisis response.
The Trusts that approach this most effectively are the ones that integrate SQL Server lifecycle management into their broader data architecture governance: maintaining a live inventory, tracking version status, triggering migration planning at a defined point before end of support, and treating cloud migration as the default destination for new and migrating workloads rather than a special-case decision.
The deadline is July 2026 for SQL Server 2016. The discipline is permanent. Legacy debt compounds when nobody is tracking it, and there is always another version approaching end of support.
Where VE3 Can Help
VE3 works with NHS Trusts to conduct structured discovery of SQL Server and wider database estates, produce risk-based remediation roadmaps, and design the cloud data architecture into which legacy databases migrate. Our work integrates SQL Server rationalisation into broader enterprise data architecture and EPR alignment programmes, ensuring migration decisions are made in the context of the Trust's target data environment rather than in isolation.
If your Trust is approaching the SQL Server 2016 deadline without a complete picture of its database estate, or is looking to design a migration programme that aligns with its wider cloud and FDP strategy, we would welcome the conversation.
.png)
.png)
.png)



